Skinny Jeans Syndrome
Lumbo-Pelvic Pain Part 3
 Meralgia Paresthetica
Meralgia Paresthetica
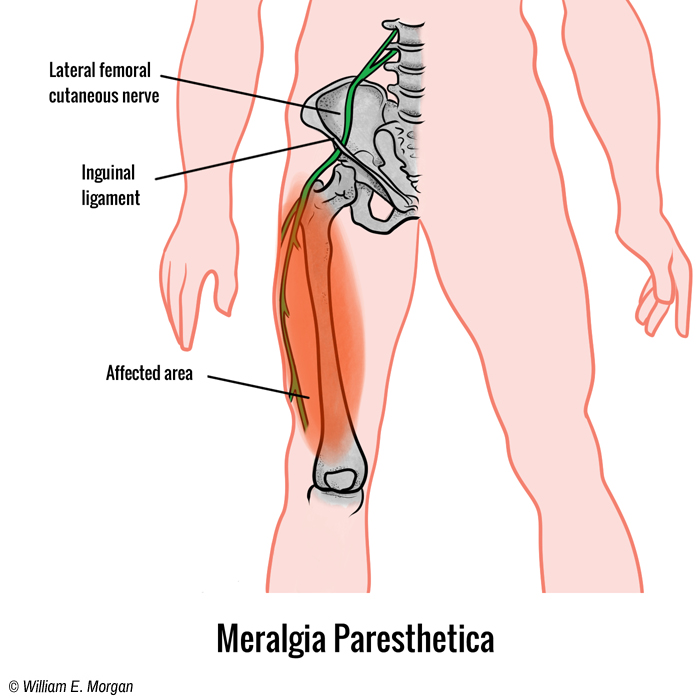
Figure 1. The lateral cutaneous femoral nerve exits the pelvis near the ASIS and under the inguinal ligament, where it is most frequently entrapped. The LCFN innervates the skin of the anterolateral thigh (shaded region).
Meralgia paresthetica (MP) is a sensory mononeuropathy which can produce pain or paresthesia of the anterior-lateral thigh. Normally it is the result of a focal entrapment of the lateral femoral cutaneous nerve (LFCN) as it travels under the inguinal ligament, but it can also be caused by external compression. This peripheral entrapment is relatively common and has been confused with nerve root lesions.
Clinical Anatomy
The LFCN, a nerve of the lumbar plexus, originates from the second and third lumbar nerves. It passes through the psoas muscle, and then traverses anterior to the iliacus muscle as it travels laterally across the pelvis. I t finally exits the pelvis near the anterior superior iliac spine (ASIS) under the inguinal ligament. The most common site of compression or entrapment is the point where the LFCN exits the pelvis under the inguinal ligament.
Since this sensory nerve innervates the skin of the anterior-lateral thigh, entrapment usually creates sensory disturbances. Studies have shown that patients with an anatomic variant which causes the LFCN to traverse closer to the ASIS are more prone to this condition.[i],[ii] This variant causes the LFCN to exit the pelvis through a tighter space.
External Causes
While anatomical variations may predispose certain patients to develop meralgia paresthetica, external pressure on the LCFN can also cause this disorder. Military body armor, police belts, workman belts, seat belts, or any external pressure compressing the LCFN, such as leaning over the hood of a car can lead to meralgia paresthetica.[iii]
Additional causes of MP which have been cited include surgery,[iv] and weight gain (even by pregnancy).[v] A study conducted at the Mayo Clinic found that diabetics were 7 times more likely to have MP.[vi]
Surprisingly, modern fashion has been the culprit in causing a recent surge in the occurrence of meralgia parethestica. Skinny jeans have been cited as the cause of an increase in the number of young people suffering from this condition. Combining skinny jeans and high heels (which anteriorly tilt the pelvis and increases the likelihood of LCFN compression) increases the likelihood of developing MP, even earning its own colloquial diagnosis: Skinny Jeans Syndrome.
Symptoms of Meralgia Paresthectica
- Burning pain of the skin (versus deep pain), which feels like a sunburn, of the anterior-lateral thigh
- Paresthesia of the anterior lateral thigh
- Numbness
- Magnification of symptoms by wearing body armor, loadbearing belts, tight belts, or “skinny jeans”
- Worse with pregnancy or obesity
Diagnosis
The diagnosis of meralgia paresthetica is almost always a clinical diagnosis, versus a diagnosis based on objective observable technology. Diagnostics such as X-ray, CT, MRI, and diagnostic ultrasound can only rule out other conditions, but they cannot confirm the diagnosis of this malady. The diagnosis of MP can be made through history, presentation, examination, and clinical deduction. Particularly helpful in making the diagnosis is the pain distribution pattern, a clearly defined cause (like the physical pressure of body armor), and a positive Tinel’s sign of the LCFN or tenderness of the nerve where it emerges from under the inguinal ligament.
Not all anterolateral thigh paresthesia is caused by LCFN entrapment. Disc herniation, spinal stenosis, and other sources of nerve root lesions of the upper lumbar (L2-L3) spine may also cause these symptoms.[vii] Nerve root lesions may exhibit motor, reflex, and MRI findings, whereas MP only has sensory findings.
The orthopedic test, femoral nerve stretch test, may be positive in both nerve root lesions and in LCFN entrapments, so this test is not beneficial in differentiating between the two conditions.
Treatment
The simplest treatment for any condition is to take away the cause. If the patient is wearing tight clothes, belts, loadbearing belts, then those should be removed. If the patient is obese, then weight loss would be the primary treatment. While there is a lack of strong evidence for any one treatment to be particularly effective, there are plenty of conservative treatments which can be started on a trial basis, and if effective, continued. Other conservative treatments could include myofascial mobilization of the inguinal ligament, neuro-mobilization techniques, stretching, pin-and-stretch techniques, passive modalities such as cold laser, and, of course, chiropractic adjustments.
Medical treatment may include drugs intended to treat nerve pain (like gabapentin), nerve blocks, neurotomy, lidocaine, and corticosteroid injections.
Three Cases
Here are how three cases of meralgia paresthetica have presented in my practice.
The first case was post-surgery. The patient woke up after surgery with burning pain in the lateral thigh. After ruling out nerve root involvement, we concluded that pressure from position or pressure (from possibly be leaned on) while the patient was anesthetized was the most likely cause. The patient’s symptoms were very superficial and could be replicated by finding the irritated LCFN through palpation as it emerged from under the inguinal ligament and tapping on it, a positive Tinel’s sign. This patient failed to respond to conservative care.
Case two: A male patient in his sixties reported with acute onset of lateral leg pain. He had recently gained weight, but continued to wear the same size trousers, which were now worn below his belly fat. The patient’s belt was worn more tightly and lower than previously. A positive Tinel’s test was noted along the lateral inguinal ligament on the affected side. The patient was encouraged to wear more loose fitting trousers, to use suspenders instead of a belt, and to lose weight. His symptoms resolved within three weeks.
Case three: A soldier presented who had worn body armor that put pressure on the anterior lateral pelvis when he rode “shotgun” in a vehicle with his right leg raised. The raised right leg allowed his elbow to rest on his thigh to enhance his ability to hold his rifle “at the ready” for long periods. The pressure of his body armor compressed the LCFN and led to MP. He responded to chiropractic adjustments and pin-and-stretch techniques, along with instrument assisted myofascial manipulation.
Conclusion
Meralgia paresthetica is a relatively common sensory mononeuropathy that in some cases may be a source of refractory pain, or it may resolve with something as simple as losing weight and wearing loose fitting clothing. It may be mistaken for an L2-L3 nerve root lesion or other neuropathies. Every musculoskeletal provider should be familiar with this condition and be able to diagnose it.
[i] Moritz T, Prosch H, Berzaczy D, Happak W, Lieba-Samal D, Bernathova M, Auff E, Bodner G. Common anatomical variation in patients with idiopathic meralgia paresthetica: a high resolution ultrasound case-control study. Pain Physician. 2013 May-Jun;16(3):E287-93.
[ii] de Ridder VA, de Lange S, Popta JV. Anatomical variations of the lateral femoral cutaneous nerve and the consequences for surgery. J Orthop Trauma. 1999 Mar-Apr;13(3):207-11.
[iii] Fargo MV, Konitzer LN. Meralgia paresthetica due to body armor wear in U.S. soldiers serving in Iraq: a case report and review of the literature. Mil Med. 2007 Jun;172(6):663-5.
[iv] Grossman MG1, Ducey SA, Nadler SS, Levy AS. Meralgia paresthetica: diagnosis and treatment. J Am Acad Orthop Surg. 2001 Sep-Oct;9(5):336-44.
[v] Mondelli M1, Rossi S, Romano C. Body mass index in meralgia paresthetica: a case-control study. Acta Neurol Scand. 2007 Aug;116(2):118-23.
[vi] Parisi TJ1, Mandrekar J, Dyck PJ, Klein CJ. Meralgia paresthetica: relation to obesity, advanced age, and diabetes mellitus.Neurology. 2011 Oct 18;77(16):1538-42.
[vii] Trummer M, Flaschka G, Unger F, Eustacchio S. Lumbar disc herniation mimicking meralgia paresthetica: case report. Surg Neurol. 2000 Jul;54(1):80-1.
 Meralgia paresthetica body armor
Meralgia paresthetica body armor
Figure 2. Body armor, police belts, and loadbearing carpenter belts can all place pressure on the lateral cutaneous femoral nerve resulting in meralgia paresthetica: pain, paresthesia, numbness, or tingling of the anterolateral thigh.