
Hint: It is not CE
Continuing education may be replaced with a new model of life long growth: Continuing Development.
There is certainly a need to ensure that doctors remain competent and their knowledge current after graduation. But what is the best way to do this? In an attempt to ensure that doctors remain competent, and that they stay abreast of current trends and advancements, licensing boards began several decades ago to dictate a prescribed number of approved continuing education (CE) class hours. But the required CE, in the form of formal didactics, is often disjointed from clinical practice. CE is often a class taken by a doctor over the weekend with the hope that some of the new knowledge may be implemented into practice on Monday morning.
Built In, Not Bolted On
Continuing development (CD) or continuing professional development (CPD) by contrast is a system intent on developing several core competencies and engraining them into the practice of the physician. CD has a goal of changing behavior and improving clinical outcomes. CD is a journey that, if done correctly, will last a lifetime and will engage the physician to learn and grow on a daily basis.
You Can Lead a Horse to Water, but…
Regardless of the intent and implementation of a continuing development program, it will fall short of its goals if the individual doctors are not invested in the process. The motivation for professional development must come from within the individual doctor. We can encourage doctors to pursue CD and to honor its concepts, but ultimately the responsibility rests squarely on the shoulders of the physician. Rules and regulations will provoke a physician to obey the letter of the law, but cannot ensure total compliance.
Characteristics of successful lifelong learners in clinical practice include:
- The drive to be a master clinician and to provide excellent patient care
- The pride in the enduring value of professional competencies and scholarly growth
- The need to expand and grow in knowledge and clinical application
Continuing development requires the heartfelt desire to grow and blossom throughout a career. Doctors must embrace the concept of lifelong learning and be knowledge seekers.
This stands in contrast to passive learning. Passive learners sit in a classroom and are taught, they are directed what to read and what to study. They do what is required of them without seeking to learn more. Passive learners can be straight A students and may be difficult to differentiate from active knowledge seekers in the classroom setting. How can we inspire passive learners to become active knowledge seekers?
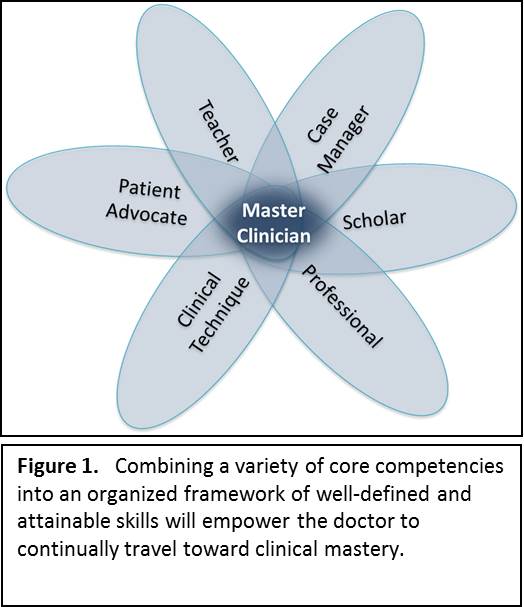 Master Clinicians
Master Clinicians
The Role of Chiropractic Colleges
Chiropractic colleges should use criteria to identify lifelong learners and actively attract and recruit these knowledge seekers. Colleges should also inspire students to continually seek knowledge rather than regurgitate lectures or board review material. They should introduce students to the tools that they will need to continue to learn and develop throughout their career. As students approach graduation, classroom-based didactics should be replaced with active clinical rotations which require students to seek knowledge while clinically active. This should translate to doctors in the field who continue to grow and learn daily through clinical encounters. Daily learning in the student clinic should be a model for daily learning throughout a chiropractor’s career.
Continuing development has many benefits for the doctor, the patients, and society. The doctor benefits from career satisfaction, and patients benefit from superior healthcare. A doctor who is continually being challenged is less likely to suffer from burnout.
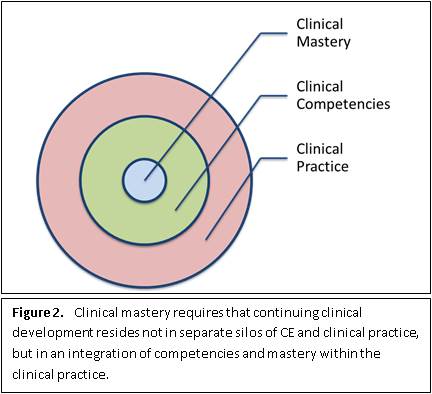 Clinical Mastery
Clinical Mastery